
Clareon® IOL with AutonoMe® Automated Delivery System
Deliver the latest evolution of control and clarity1-3
Clareon® IOL with AutonoMe® Automated Delivery System
Deliver the latest evolution of control and clarity1-3
Designed for precise IOL delivery with easy, intuitive control

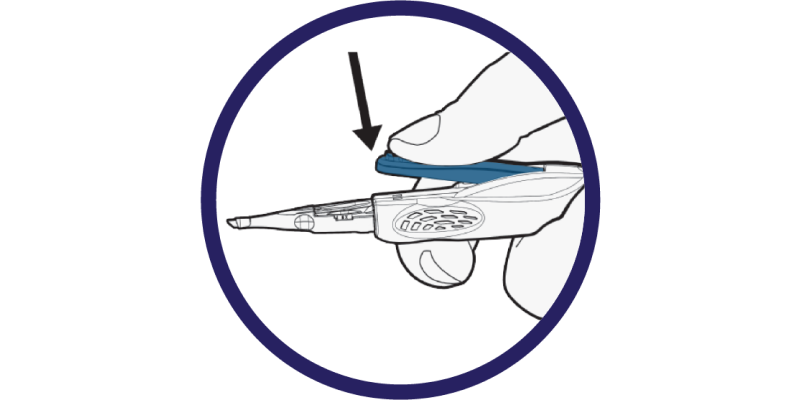
Easy: Single-handed
control of IOL delivery1,4*,†
- Innovative, automated CO2-powered delivery mechanism
- Integrates a responsive speed control lever
- Precisely start, stop and vary the speed of delivery at any time

Intuitive: Designed for comfortable, ergonomic hand positions4
- Entire device is optimized for intuitive control of IOL delivery

Control: Designed to enable precise delivery into the capsular bag4
- Designed to protect incisions as small as 2.2 mm with a proprietary depth guard
- Designed to provide full IOL visibility during delivery with a 3 mm nozzle tip
Ready to implant in just 3 steps1‡,§
Once the IOL is in the pause location, the lens should be implanted within 1 minute.

Step 1:
Fill with an Alcon-qualified viscoelastic

Step 2:
Remove the lock-out assembly
Step 3:
Advance the plunger to fold the IOL up to the pause location
Available with the Clareon® Monofocal IOL
Clareon® Monofocal IOLs provide exceptional clarity**, allowing you to confidently deliver the long-lasting refractive outcomes that your monofocal patients expect.3,5,6
Exceptional Clarity that Lasts5††
Delivers among the lowest levels of glistenings, SSNGs, and surface haze.3†† In long-term clinical studies, Clareon® IOLs were reported as glistening-free over 3 and 9 years.3,7,8††
Proprietary Precision Edge Design9
Proprietary edge curvature designed to help reduce PCO and edge glare9
Superior Axial Stability10-12‡‡
Fibronectin helps bind the material to the capsule, anchoring the lens in place to help reduce PCO and improve stability.9,12,13

Optical Design with Proven Performance5,9,10,§§
Clareon® and AcrySof® share the same -0.2µm aspheric design resulting in improved depth of focus with a fully usable 6mm optic.9,10,§§
Available on Clareon®: Alcon’s most advanced IOL biomaterial to date

![]()
* Based on feedback from 112 surgeons, following implantation of Clareon® IOLs in porcine eyes using the AutonoMe® delivery device via clear corneal incisions.
† Based on ranking of ease of use compared to current Alcon delivery device; options included “easier” (68%), “the same” (28%), and “more difficult” (4%).
‡ For full preparation and administration information, please refer to the directions.
§ For Use for Clareon® IOL and AutonoMe® Delivery System.
** Based on in vitro examinations of glistenings, surface haze and SSNGs.
†† Defined as Modified Miyata grade 0, <25mv/mm2 over 3 years (n=138), and over 9 years (n=20), respectively.
‡‡ In vitro comparison with enVista^ MX60, TECNIS^ 1-Piece, and Vivinex^ XY-1 for axial displacement (n=5 IOLs per group, +20.0 D). Axial displacement was measured in vitro in deionized water at 35° C and was measured at multiple compression diameters (11.0, 10.5, 10.0, 9.5, and 9.0 mm). Games-Howell pairwise comparison (10 per IOL) (p=<0.005 for Clareon CNA0T0 versus enVista^ MX60, TECNIS^ ZCB00, or Vivinex^ iSert XY-1 at all compressions)
§§ Clareon® and AcrySof® share the same -0.2um aspheric design resulting in improved depth of focus.
^ Trademarks are the property of their respective owners.
IMPORTANT PRODUCTS INFORMATION - CLAREON® MONARCH® IV IOL DELIVERY SYSTEM
CAUTION: Restricted by law to sale by or on the order of a physician.
INDICATIONS:The Clareon® Monarch® IV IOL Delivery System is for implantation of qualified Alcon foldable IOLs. No unqualified lenses should be used with the Clareon® Monarch® IV IOL Delivery System.
WARNINGS / PRECAUTIONS: Consult the product labeling for the complications associated with the Clareon® Monarch® IV IOL Delivery System used in conjunction with cataract surgery and IOL implantation.
HANDPIECE PRECAUTIONS:
- A high level of surgical skill is required for intraocular lens implantation. The surgeon should have observed and/or assisted in numerous implantations and successfully completed one or more courses on intraocular lens implantation before attempting to implant intraocular lenses.
- Read all instructions prior to use.
- The handpiece is non-sterile and must be cleaned and sterilized prior to each use (refer to Handpiece Preparation section of Instructions for Use). Failure to properly sterilize handpiece could result in serious infection (e.g., endophthalmitis and systemic infection).
- Use of hydrogen peroxide may discolor titanium instruments.
- Mixing titanium and stainless-steel instruments during sterilization may result in discoloration of the instruments.
- If a patient with a prion-related disease undergoes a procedure which, in the medical opinion of the physician, poses a high risk of instrument contamination, the instrument should be destroyed or processed according to local requirements.
ATTENTION: Reference the Directions for Use labeling for each IOL for a complete listing of indications, warnings and precautions.
IMPORTANT PRODUCTS INFORMATION - CLAREON® FAMILY OF IOLS
CAUTION: Restricted by law to sale by or on the order of a physician.
INDICATIONS:The family of Clareon® intraocular lenses (IOLs) includes the Clareon® Aspheric Hydrophobic Acrylic and Clareon® Aspheric Toric IOLs, the Clareon® PanOptix® Trifocal Hydrophobic IOL, Clareon® PanOptix® Toric, Clareon® Vivity™ Extended Vision Hydrophobic Posterior Chamber IOL and Clareon® Vivity™ Toric IOLs. Each of these IOLs is indicated for visual correction of aphakia in adult patients following cataract surgery. In addition, the Clareon® Toric IOLs are indicated to correct pre-existing corneal astigmatism at the time of cataract surgery. The Clareon® PanOptix® lens mitigates the effects of presbyopia by providing improved intermediate and near visual acuity, while maintaining comparable distance visual acuity with a reduced need for eyeglasses, compared to a monofocal IOL. The Clareon® Vivity™ lens mitigates the effects of presbyopia by providing an extended depth of focus. Compared to an aspheric monofocal IOL, the lens provides improved intermediate and near visual acuity, while maintaining comparable distance visual acuity. All of these IOLs are intended for placement in the capsular bag.
WARNINGS / PRECAUTIONS: General cautions for all Clareon® IOLs: Careful preoperative evaluation and sound clinical judgment should be used by the surgeon to decide the risk/benefit ratio before implanting any IOL in a patient with any of the conditions described in the Directions for Use that accompany each IOL. Physicians should target emmetropia, and ensure that IOL centration is achieved. For the Clareon® Aspheric Toric, PanOptix® Toric and Vivity™ Toric IOLs, the lens should not be implanted if the posterior capsule is ruptured, if the zonules are damaged, or if a primary posterior capsulotomy is planned. Rotation can reduce astigmatic correction; if necessary lens repositioning should occur as early as possible prior to lens encapsulation. For the Clareon® PanOptix® IOL, some visual effects may be expected due to the superposition of focused and unfocused multiple images. These may include some perceptions of halos or starbursts, as well as other visual symptoms. As with other multifocal IOLs, there is a possibility that visual symptoms may be significant enough that the patient will request explant of the multifocal IOL. A reduction in contrast sensitivity as compared to a monofocal IOL may be experienced by some patients and may be more prevalent in low lighting conditions. Therefore, patients implanted with multifocal IOLs should exercise caution when driving at night or in poor visibility conditions. Patients should be advised that unexpected outcomes could lead to continued spectacle dependence or the need for secondary surgical intervention (e.g., intraocular lens replacement or repositioning). As with other multifocal IOLs, patients may need glasses when reading small print or looking at small objects. Posterior capsule opacification (PCO), may significantly affect the vision of patients with multifocal IOLs sooner in its progression than patients with monofocal IOLs. For the Clareon® Vivity™ IOL, most patients implanted with the Vivity™ IOL are likely to experience significant loss of contrast sensitivity as compared to a monofocal IOL. Therefore, it is essential that prospective patients be fully informed of this risk before giving their consent for implantation of the Clareon® Vivity™ IOL. In addition, patients should be warned that they will need to exercise caution when engaging in activities that require good vision in dimly lit environments, such as driving at night or in poor visibility conditions, especially in the presence of oncoming traffic. It is possible to experience very bothersome visual disturbances, significant enough that the patient could request explant of the IOL. In the parent AcrySof® IQ Vivity™ IOL clinical study, 1% to 2% of AcrySof® IQ Vivity™ IOL patients reported very bothersome starbursts, halos, blurred vision, or dark area visual disturbances; however, no explants were reported.Prior to surgery, physicians should provide prospective patients with a copy of the Patient Information Brochure available from Alcon informing them of possible risks and benefits associated with these IOLs.
ATTENTION: Reference the Directions for Use labeling for each IOL for a complete listing of indications, warnings and precautions.
REFERENCES:
- 1. Clareon® Aspheric Hydrophobic Acrylic IOL with the AutonoMe® Product information DFU.
- Mastropasqua L, Toto L, D'Ugo E, et al. In vivo and in vitro results of an automated preloaded delivery system for IOL implantation in cataract surgery. Int Ophthalmol. 2020;40(1):125-134.
- Werner L, et al. Evaluation of clarity characteristics in a new hydrophobic acrylic IOL in comparison to commercially available IOLs. J Cataract Refract Surg. 2019;45(10):1490-1497. doi:10.1016/j.jcrs.2019.05.017.
- Alcon Data on File, 2017.
- Lehmann, R., Maxwell, A., Lubeck, DM, Fong, R., Walters, TR, Fakadej, A. Effectiveness and Safety of the Clareon® Monofocal Intraocular Lens: Outcomes from a 12-Month Single-Arm Clinical Study in a Large Sample. Clin Ophthalmol. 2021;15:1647-1657. Published 2021 Apr 20.
- Alcon data on file, 2019.
- Oshika T, Fujita Y, Inamura M, Miyata K. Mid-term and long-term clinical assessments of a new 1-piece hydrophobic acrylic IOL with hydroxyethyl methacrylate. J Cataract Refract Surg. 2020 May;46(5):682-687.
- Maxwell A, Suryakumar R. Long-term effectiveness and safety of a three-piece acrylic hydrophobic intraocular lens modified with hydroxyethyl-methacrylate: an open-label, 3-year follow-up study. Clin Ophthalmol. 2018;12:2031-2037.
- Das KK, Werner L, Collins S, Hong X. In vitro and schematic model eye assessment of glare or positive dysphotopsia-type photic phenomena: Comparison of a new material IOL to other monofocal IOLs. J Cataract Refract Surg. 2019;45(2):219-227.
- Clareon® Toric Directions for Use.
- Alcon Data on File, 2017.
- Lane S, Collins S, Das KK, et al. Evaluation of intraocular lens mechanical stability. J Cataract Refract Surg. 2019;45(4):501-506.
- Alcon Data on File, 2017.